When Cycling Hits a Nerve: Cyclist's Palsy
- golabiromtin
- Jun 6, 2025
- 4 min read

Updated: Jun 23, 2025
By Romtin G.
Introduction
Cycling is renowned for its low-impact, beneficial nature, which helps improve muscle strength, coordination, and endurance while also reducing stress levels. However, like any repetitive activity, it carries a unique set of physical risks. One of the most common yet underrecognized is Cyclist’s Palsy (or ulnar neuropathy). This condition arises from prolonged pressure on the ulnar nerve at the wrist or hand, causing numbness, tingling, and weakness in the ring and pinky fingers. A lot of cyclists mistake this for general hand fatigue, but Cyclist’s Palsy can reduce one’s grip strength and control, especially for long-term riders or those who ride bikes with poor ergonomics. As more people take up cycling as a hobby, the need for thorough answers and awareness must grow to better inform the public on this injury. This article explores the physiology, risk factors, treatment, and current research surrounding Cyclist’s Palsy.
Physiology
Let’s start by getting an idea of the what, where, and why of Cyclist’s Palsy.
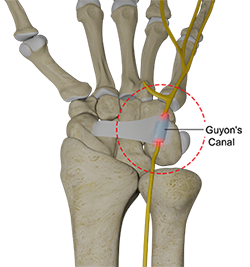
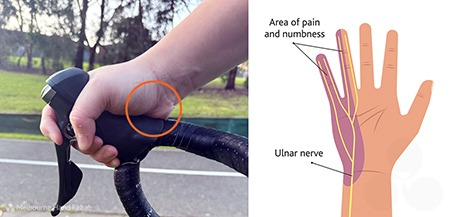
Cyclist's Palsy is a condition that occurs when the ulnar nerve is compressed. The ulnar nerve is the nerve that runs along the long bone on the pinky side of the arm (ulna), and branches off into two sections that ultimately provide sensory and motor functions to the pinky and half of the ring finger. The ulnar nerve passes through a tunnel/passageway called Guyon’s Canal, formed by the space between two wrist bones. It is mostly at this spot that the ulnar nerve gets compressed.
But what bad habits can cause this compression to occur? The condition can result from many different stressors, but all of them tie back to too much pressure on the ulnar nerve region: weak core muscles (and thus an excess application of pressure to the hands), rough terrain (vibrations exacerbate pressure), high seat or low handlebars, over-inflated tires (more vibrations), maintaining a hyperextended wrist position for a long time (stresses sensitive structures around the ulnar nerve), and so many more. This eventually results in tingling, numbness, pain, weakness, and in severe cases, complete paralysis of one’s pink and ring fingers (though this is very rare and one would probably know something is wrong before getting to this point). The reason nerve compression causes these symptoms is that compressed nerves can’t send/receive signals as accurately or efficiently. Resultingly, the abnormal signals that the nerve sends are interpreted by the brain as sensations of pins and needles, numbness, etc. The compression may additionally affect blood vessels that supply the nerve, potentially causing it to become ischemic (lack of oxygen) and further contributing to pain and tingling.
Treatment and Current Research
Fortunately, dramatic intervention is rarely required to treat this injury. The most obvious treatment is rest and reduced cycling, which would allow the nerve to recover and repair any damage caused by the compression. Once one has recovered, it is important to readjust their bike to ensure the injury doesn’t happen again—that means changing the seat height and angle, changing the handlebar position, or any other adjustment that would improve ergonomics. Padded gloves are also a great option, as they help with cushioning and distributing natural pressure throughout the hand. Sometimes, the compression results in an inflammatory response that, in turn, causes more nerve compression, so NSAIDs like ibuprofen or aspirin can help reduce inflammation and pain. If these don’t help, steroid injections can be beneficial as they reduce the immune response that produces the inflammation. In rare cases, these treatments are ineffective, so decompression surgery must be performed to relieve stress on the nerve. This involves making a small incision, removing any structures (ligaments, bony spurs, etc.) that contribute to the nerve compression, and closing up the incision.
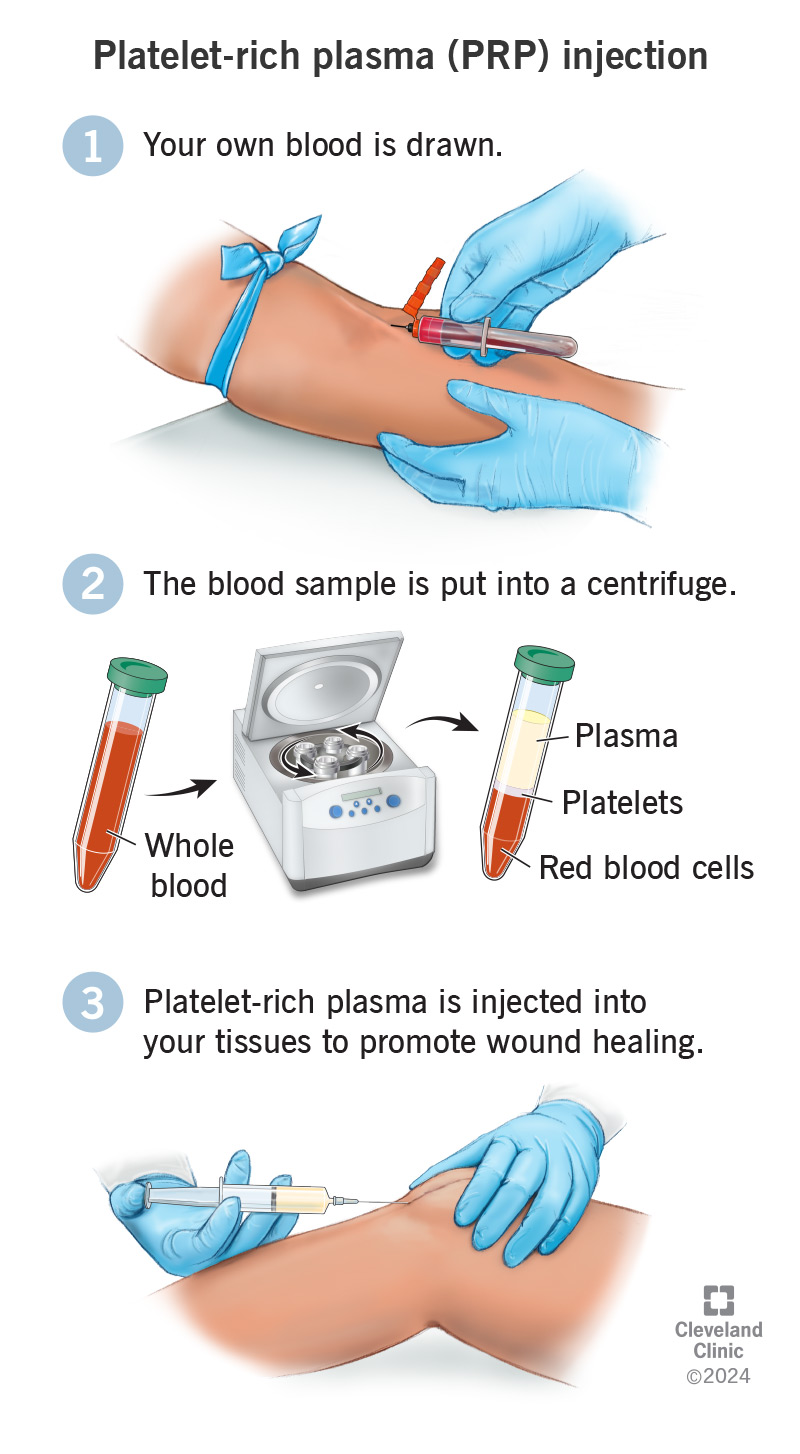
Now, onto current research! Since I’m very interested in stem cells/regenerative medicine/tissue engineering, I will focus this paragraph on these topics. Unfortunately, with nerve compression, nerve damage is almost inevitable, so even though the treatments above may relieve symptoms, they don’t address the root cause. That’s where stem cells come into play! Stem cells are undifferentiated cells that can develop into various cell types, so injecting stem cells into affected areas can promote nerve regeneration! However, one major current obstacle is controlling the exact type of cell these stem cells differentiate into when manufacturing them in the lab, but once we overcome that, we could do so many cool things! Another type of therapy is called Platelet-Rich Plasma (PRP) Therapy, which involves drawing the patient’s blood, concentrating the platelets, and then reinjecting the blood serum back into the affected area. In some cases, the myelin sheath (fatty tissue that conducts electricity and speeds up the signal) of the nerve can be damaged from compression. The PRP is filled with growth factors that greatly accelerate healing, and it can help with rebuilding the myelin sheath! PRP Therapy can treat many disorders beyond Cyclist’s Palsy, such as osteoarthritis, acute muscle injuries, hair loss, skin rejuvenation, and much more!
Conclusion
Thank you for reading my article—stay posted for more content in the future!
Sources